

Date: 24th February 2021
To watch the recording click here
Register to download the webinar presentation.
Transcript
LTC Facilities – Design Dinosaurs
Facilitated by Irving Stackpole. With architect Kevin Kozak, interior designer Laura Sheehan and Garth Johnson of Cutler Associates.
Irving Stackpole
Thank you all for coming today I am very flattered that so many of you decided to participate in this program. We’ve chosen the topic today to zero in on several areas. One is to talk about in a constructive way possible during this very difficult covid related pandemic that we’ve uncovered problems with regards to long term care. We’ve realized that there are barriers to making changes. It’s recognized that there are some learnings. Most importantly, we want to focus on realistic next steps. My colleagues at Cutler Associates will go through very realistic approaches to new construction of new construction and major renovations and additions, selected renovations. Then we’ll have some time for Q&A.
Importantly, the problem revealed in long term care and in particular the skilled nursing environment during the covert’s pandemic, the particular learning has been that the physical properties and the programs weren’t up to snuff. There were problems even causing one author here for The New Yorker magazine publication to declare that the American nursing home was a design failure and colleagues like David Grabowski anticipating big, big changes coming to long term care.
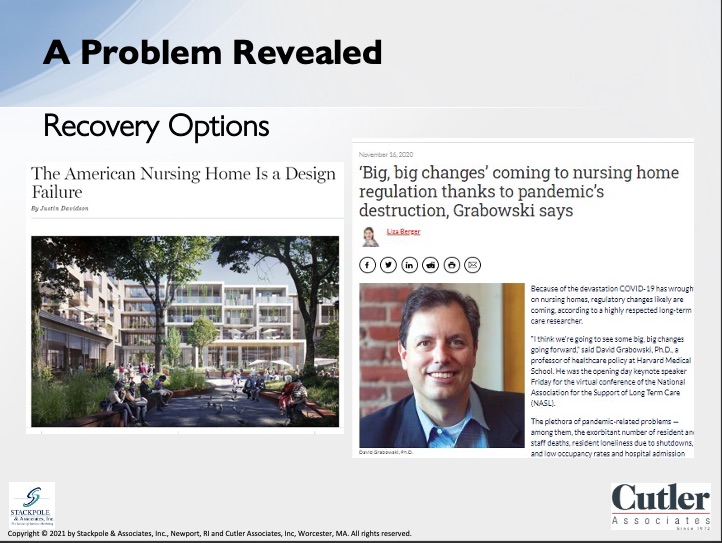
The reasons for this are pretty simple, that while the population in long term care in the United States is a fraction of 1% of the adult population overall, by some calculations, as much as 42% of the deaths occurred in congregate long-term care. So, what’s those big changes we have yet to see? But certainly, the subject is afoot and important for all of us in these problems in this domain. There are a set of issues that need to be dealt with. The issues include the structures which were going to be focusing on in this session, but also include programs, the soft programs, the systems and the care programs that are in place in these structures to address the needs of the populations we’re in, we’re hoping to serve. Of course, there’s issues around technology and information, staffing, culture and outcomes as well as economics.
The focus of this particular program will be on the structures, the properties, the physical design, the equipment, the gear handling equipment, the colleagues at Cutler will address so, so much more expertly than I can have been very seriously challenged by the pandemic. The fact is that most of the nursing homes in the United States were built between 1964 and 1975 that were modeled on hospitals. And if you think about it, that means that the architects and planners who were building the nursing homes in the United States were themselves born in the 1920s to 1930s, and they were designing for people who were born in the 80s, 90s to the 90s. The turn of the century was very, very different population than what we had this time.
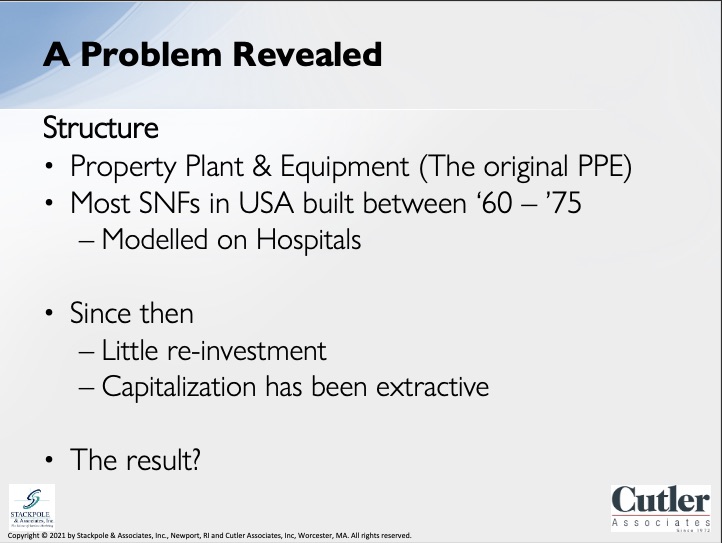
Since then, unfortunately, there’s been very little reinvestment and most of the capitalization in this sector has been extracted and the money has gone elsewhere. So the result is that the pandemic ripped through nursing homes and congregate care structures in the United States, resulting in a very difficult that’s even an understatement, resulting in the devastation staff and residents and their families being very deeply affected by the crisis is a terrible thing to waste.
What is it that we need now? What we need an array of infrastructure. We need an array of properties. We need large properties like newer college dormitories. We need medium sized properties like purpose-built assisted livings today, which, by the way, took market share away from skilled nursing because it was a more attractive product. We need small properties because some people prefer that. If you think of what are referred to today as McMansion or the Golden Girls model, where people related or somewhat related are living together, but the idea is that we need to revisit what it is. Our physical environments are built, environments need to be today. And that’s why I’m so grateful that our colleagues from Cutler Associates have agreed to speak to us today.
Garth Johnson
Covid-19 revealed issues with skilled nursing facilities and the barriers to fix them are perhaps more recognized now than they’ve been in decades. We all know that there’s an industry wide big picture that needs to be addressed. And here are some of the things we all know. Our problems, as Irving mentioned, there are some possibilities, hopefully, that will come out of the pandemic. And here in Massachusetts, we were hit harder than most places in the US. There are thirty-eight thousand residents in long term care facilities out of a total overall state population of seven million.
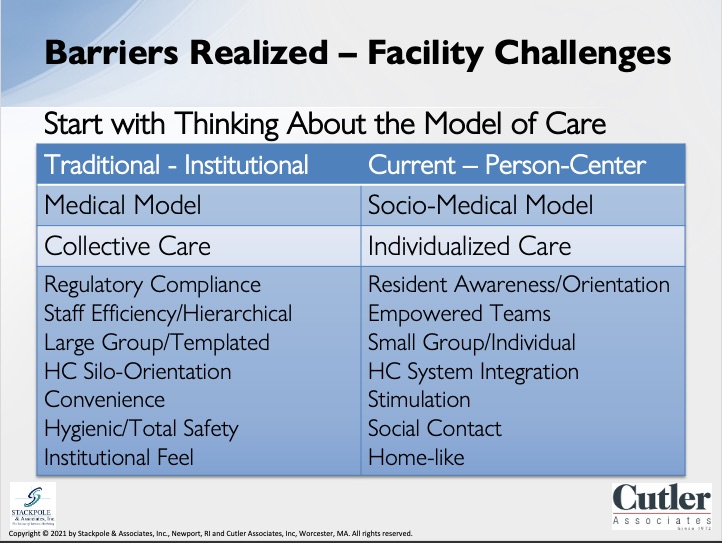
In Massachusetts, yet the first wave of that and the first wave of the pandemic, this, a group accounted for 63% of the covid-19 deaths statewide. And so, Irving’s percentage is related to 42%. Massachusetts was 50% higher than that. So, this has been a huge, huge issues. And so, in my mind, there’s at least two wakes up realizations that may be helpful to create change as we look forward. The first one is that stiffs aren’t going away and the second with this kind of impact that’s occurred and frankly, just the sheer number of deaths and problems, it’s becoming increasingly unacceptable to ignore problems any longer by anyone, whether that’s within the health care systems or as a state or as a country. The key point to realize as we start to think about what to do and start looking forward to changing is to realize the starting point is not with our buildings, but we need to first look at the model of care that skilled nursing facility organizations want and need to provide. And many of today’s nursing homes says again, Irving mentioned, were constructed to serve a medical model of care that is now largely obsolete. The shift to person centered care has been going on for little years, and there’s an emergency community-based care model that’s not outlined here. That’s the basis of green house and small house and other models like that. So, the point I’m trying to make is, is that if we’re going to revolutionize our skilled nursing facilities, we have to start with the care and the service outcomes that we’re looking for.
Also, as we consider how to move forward, it’s important to recognize the very practical and considerable barriers that we face with many of our existing buildings. Here’s a description of what many of the nineteen sixties and seventies era buildings are like now. Let me just take one example from this list. Back then, acceptable, acceptable practice was to count on operable windows for fresh air, and that doesn’t work too well here in New England at this point. And but from an infection control standpoint, covid exposed really how detrimental this layout is for indoor air quality. The way that older HPC systems actually work is that air is pumped into the corridors.
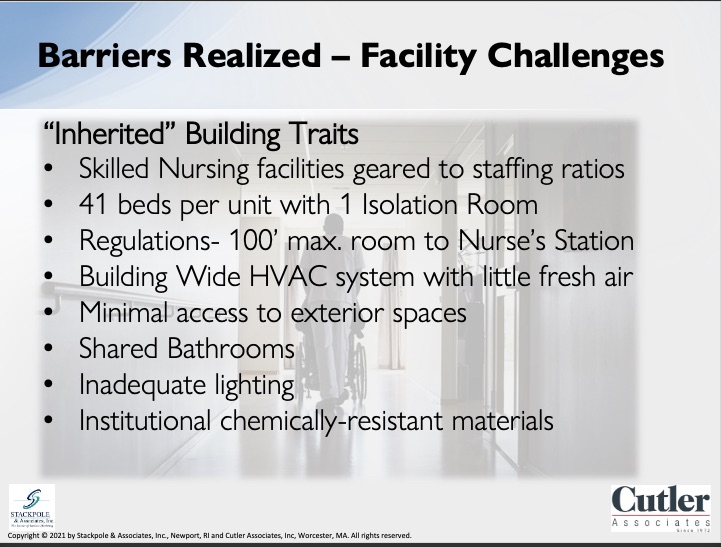
The resident rooms have baseboard rather than air system. But what they do have is they have a bathroom exhaust fan. And so, as a result, air flows from the corridor into the resident room because the bathroom exhaust fan pulls in the air along with any contaminants from the corridor into the room. The setup is obviously a problem when it comes to having a virus that spread through aerosols that hang in the air. I realize that many facilities probably have a group that we’re talking to today are at different places, perhaps you’ve been upgraded, and you have different systems, but thinking probably what we’re really suggesting is that the starting point is the first consider the care model and then the next step is to examine the barriers that are inherent in your buildings as you consider improvements and then get very specific about both. Or to phrase it as a question, what does your organization want to do first?
Kevin Kozak
I’d like to start with the CDC hierarchy of controls. This is a systematic approach to infection control by limiting exposure to hazards, following this hierarchy leads to the implementation of inherently safer systems. The basic concept is that the control method at the top of the graphic is potentially more effective and provide greater protection than those at the bottom. However, they also tend to be the most difficult and expensive to implement. Engineering controls, which you will see in the center, are generally favored by controlling exposures because they are designed to remove the hazard at the source before it comes in contact with staff and residents. You will notice the PPY is only one part of the solution and is the least effective at the bottom of the graphic. Thinking about operations is critical to the success of the program.
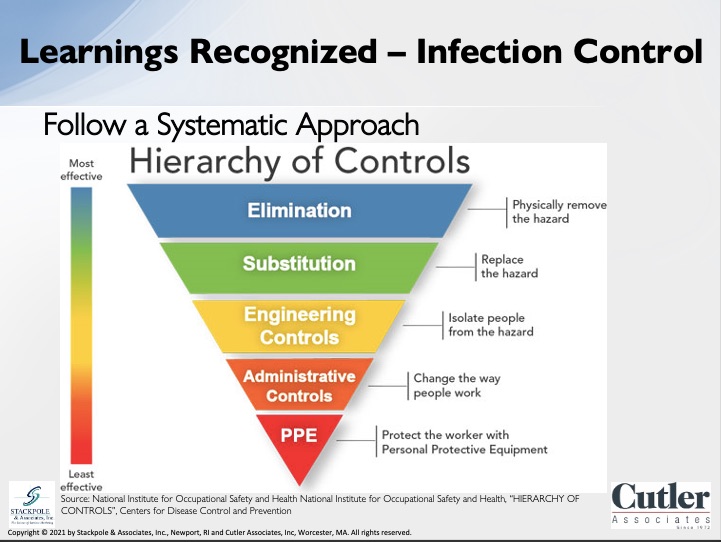
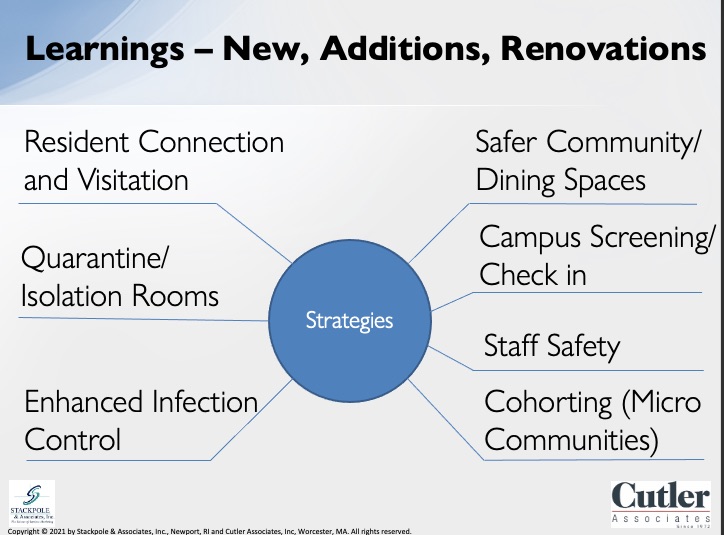
One example is a CCRC that we are local to us is noted over four hundred and fifty people every day access their campus and they have eighty-five points of entrances to their buildings. Understanding how to monitor and control access is every bit as important, if not more important than PPY. So, learning’s recognized, I’d like to discuss specific covid solutions that can be implemented on our buildings and campuses, these are areas that our clients have described as their concerns, and these concerns have informed the following solutions. Quarantine or isolation rooms are private rooms for new resident movements or positive tests. They include enhanced HVAC systems for staff safety by utilizing increased fresh air that Garth mentioned and other measures such as negative pressures. This issue was especially critical with regulations requiring 14-day quarantine for any new resident. Is resident connection and visitation, this is another important concept due to the isolation that was felt by so many residents at the beginning of the pandemic. Ideally, these rooms would be adjacent to the front entrance and they would include two different entrances, one for residents and one to visitors to minimize the chance of infection. They would also include the HBC enhancements that I had previously mentioned. With quarantine rooms. Next hour, safer community and dining spaces, strategies for this include the creation of smaller dining and activity spaces, which would include HVAC system upgrades.
Also, by keeping residents together in smaller clusters, rather than have them leave the neighborhood for communal dining and communal spaces, we can decrease the possibility of transmission and infection. Campus screening and checking procedures, as described by my previous CCRC example, it is critical to understand who is coming and going into facilities and campuses. Various strategies here can be employed to monitor visitors, which include limiting access points to campus and remote temperature checks. However, understand that larger communities that may be more difficult and could require multiple checking stations. Staff safety, we have all seen how important it is to keep staff. Set safe and healthy, given the challenges that many centers face with keeping staff people, is, of course the predominant element that we have seen throughout pandemic. But we should consider how staff exit and enter the building and understand how staff overlaps that shift changes. This is especially critical due to the fact that many staff work at multiple facilities. Strategies here include gowning, areas for PPY and places for staff to shower after their chests.
Cavorting in micro communities similar to the small House contest concepts that Garth has previously mentioned, these have been shown to greatly reduce infection transmission. We can incorporate small communities of residents and staff to create bubbles which help decrease the risk of infection. And finally, enhanced infection control measures can be introduced at the micro and macro levels within our buildings and can help reduce the spread of infection. Now, I’d like to expand on how we can use these systems on our projects to help with infection control and improve wellness in general. There are several broad strategies which can be implemented on new and existing buildings, we like to think of them in three buckets.
First, optimize existing systems where you can, particularly if they are used for ventilation strategies, include increased ventilation and filtration, air sanitization and humidification. Second, we use point of view systems that do not need to be implemented on a building wide scale. These concepts include adding or altering existing systems for point of view solutions, as well as negative air for quarantine and visitation rooms, for example. And just last week, we found a new solution for these types of systems which you can contest. Contact us after the present, find out more about. And third, finally take advantage of the opportunities when you have them. This could be a renovation edition or a new building, we would recommend incorporating multiple strategies depending on the project scope. And that way we can use these opportunities to make the largest impact. Here are some examples of how he can implement these broad strategies in our buildings and projects, increased ventilation, as Garth mentioned, the old system used operable windows, which is an ideal or practical.
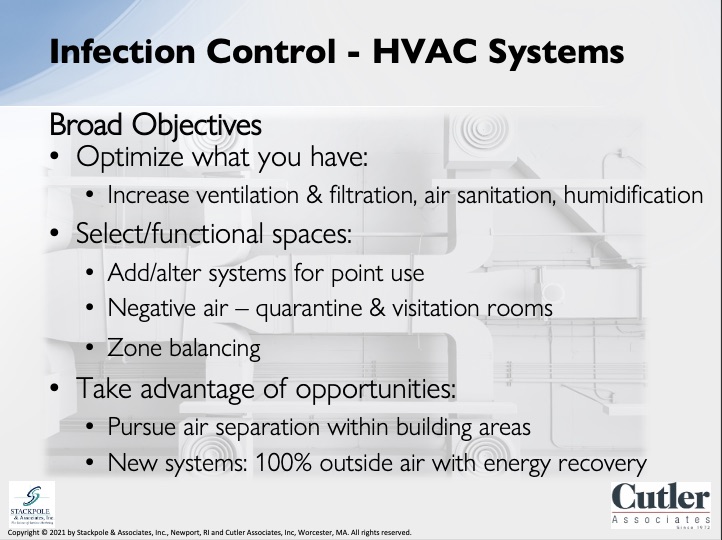
New designs increase ventilation and air changes within all areas of the building, not just common spaces, but resident rooms as well. One example of the strategy would be the creation of specialized rooms, just as visitation or the private isolation rooms I previously mentioned. This could also include system pressurization, which includes creating negative pressure, which would keep the air from being circulated to other parts of the building. We can also create zones within the building to help keep hazards out, going back to the CDC hierarchy of controls. This concept creates public, semipublic and private zones within the building, finally, new or replacement HVAC systems should include 100 percent outdoor air, greater air changes, and also a review and understanding of airflow patterns within the building to eliminate cross contamination. The greatest way to maximize the effect is to utilize several strategies to provide the most comprehensive solutions for our problem.
Laura Sheehan
Thank you, Kevin. So, when designing a space, especially in senior living in health care, it’s important to create a space that’s functional and safe as well as beautiful. So, I’m going to focus on some characteristics that provide an easier means of cleaning in these spaces. The first is durability. You want to make sure that all of your surfaces and materials are extremely durable. You don’t want anything to chip or crack. You also want fabrics and textiles to be extremely durable as well. So, there are no rips or tears. These imperfections can be a breeding ground for germs and bacteria. Another is clean ability. You want your surfaces and materials to withstand hospital grade cleaning agents, and your fabrics must also be fluid and stain resistant as well as non-porous. These materials should have the ability to suppress microbial growth as well. So, fabrics and would typically hold a lot of moisture and are likely to support microbial growth. Metals and hard plastics are less likely to support this growth and those are more preferred materials in these spaces. Surface porosity is another one. You want to eliminate the use of Cotton’s nylons and other porous substrates microorganisms have been shown to survive on. So, you want to get rid of those. You also want to eliminate seams. Any time you have seams, it can be a breeding ground for bacteria and germs. So, it’s important to eliminate them when possible or completely seal the seams when eliminating isn’t an option. So, an example of this would be if you’re using sheet vinyl in a bathroom, you typically have a seam in your sheet vinyl. So, you want to either heatwave that or chemically seal it. Another good practice is to flash that sheet vinyl up the wall to create a really impervious barrier for germs and bacteria.
So, in addition to creating a safe and functional space for residents and staff, it’s also very important to create beautiful, esthetically pleasing spaces as well. So, I’m going to touch on a few design trends that I like to follow. So, the first is transitional excuse me. The first is creating an updated and fresh look. So obviously, we want to create a new space. We want it to follow current design trends. We want to make the space feel new and fresh for the residents. But we also want to create this nice new space for staff as well. And this helps in terms of marketing. When you’re touring families through, potential residents through and they see this brand new updated fresh space, they’re going to want to live there. Another design concept is transitional design. This, in a nutshell, blends traditional design with modern design.

So, it’s a great concept for all areas of design, including new construction, but it’s especially great for renovations and additions. It gives that space an updated and fresh look, but it also allows the space to be cohesive with the rest of the building and or the campus as well. The next topic is color and lighting. So, we could have a whole another webinar on just color and lighting.
There have been so many studies on color and lighting. I’m just going to touch on a couple key points that we see. So, you want to take into account the population. For example, a memory care unit would have different lighting and a different color scheme compared to a traditional skilled nursing center.
In all cases, it’s very, very important to bring in as much natural light as possible into these spaces. Which brings me to my next point. Bringing the outside in. This is one of my favorite concepts. You can see the font in the photos on the slide. We’ve done this in several different areas. So, the concept is basically taking naturalistic materials and elements and incorporating them into the interior design. So, you can see in these photos, there’s a stone surrounded the fireplace. We use a decorative wood ceiling throughout the space and organic and floral patterns on the upholstery. So, this gives a sense of warmth and creates a connection to the earth, the stone, the wood, the textiles on the furniture. All of these elements are reminiscent of the outdoors. They create a serene and calming environment for the residents and staff. And now I’d like to turn it over to Kevin.
Kevin Kozak
Now that we understand the concepts, we must ask, how do we implement what we learned? We must not waste the painful lessons that the pandemic has taught us. We start with the areas of focus that I discussed earlier, and then we will review some examples. First, we start with the new or replacement buildings. Strategy is to align with each provider’s priorities based on the model of care that Garth described earlier, new buildings provide the greatest opportunity to incorporate as many solutions as concepts as possible. They could include small, newer models, such a small house concept, or we could incorporate these concepts into larger centers, both can be effective if implemented properly.
For example, various infection control measures can be implemented and can include things such as visitation rooms, cohort’s enhanced measures or other infection control measures with materials. Here are some examples. One example is the small house greenhouse model, these photos are from a greenhouse project that we completed, which was a fairly typical greenhouse with 12 private rooms. However, we are also in the early planning stages of a project that has shifted from separate greenhouses to a congregate building with five neighborhoods and an information administration wing, but still utilizes many of the greenhouse concepts for their model of care and their design. Some of the reasons to include small house concepts relate to the relate to the fact that these models have been better for crisis management due to their smaller size and populations, the rate of covid and small house and green houses were less than half the rate in traditional skilled nursing centers nationwide, and their death rate was less than 30 percent in small house greenhouse models.
Some of the reasons include fewer staff coming and going through the building. Residents also felt less isolation due to the small community environment, and they were more engaged. And lastly, if there was an exposure, the controls that are in place created a safer environment. Here’s another example. We can still implement these concepts and measures in a larger design.

This is a 80 to bed new skilled nursing center currently in design, which implements many of the same strategies. It includes more private rooms, which will help for quarantine and isolation, and it includes the cohort in concept. There are two floors, each with their own common dining and activity areas. This will limit the number of people that are going back and forth to each neighborhood. And there are no communal dining areas, as with more traditional designs, it also includes enhanced HVAC systems such as fresh air to all resident rooms, and each neighborhood also has its own exterior space fire, a garden or deck. Studies have shown that is over 18 times safer to be outside compared with being indoors, and they have also noted how access to the area is very important for residents. Laura mentioned that earlier with the concept of bringing the outside. Our next category are major renovations and additions.
The impact and strategies will likely depend on the size and scope of your renovations, but they are still opportunities to implement several concepts. For example, we could still move away from communal dining areas and activity rooms. Often large projects include HPC system upgrades or replacements. Or we could include localized HP and HP enhancements, such as visitation or quarantine rooms. Here are some examples. This is an example of a renovation project that’s currently in design, the existing, which you will see on the left is a more traditional model. The new design on the right incorporates cohort and concepts to the creation of a small community with private rooms. It also includes larger common spaces and dining specific to this group of residents, as well as direct access to an exterior courtyard. Here is another example of a renovation project, which includes similar concepts to the prior examples, this includes co hosting as well as access to the exterior as well as private rooms.
Another added measure includes enhanced HPC systems through the use of increased ventilation. We have also created a visitation room off the main neighborhood lobby, which we have highlighted on the right. This allows visitors to see family members without actually entering the neighborhood. And finally, select renovations offer the smallest ability to impact major changes, however, by being strategic with these opportunities, we can still be impactful.
Examples could include finish upgrades, which incorporate materials which provide better infection control, such as the ones that more Laura mentioned previously. Other examples could include visitation or quarantine rooms, rooms with enhanced measures. Here are some examples of these. We have this example; we have recently been hired to create visitation rooms at three facilities for one over the highlighted example. On the left shows a visitation room adjacent to the main lobby with different access points for residents and family members, which will reduce infection. This project also includes enhanced HVAC systems to assist with reducing infection. And our final example is an existing facility where we are looking at ways to improve staff safety. This concept is to create a separate entrance and exit for staff to minimize the interaction and shift changes. You will see on the left the entrance to the facility, which leads to the lounge and bathrooms and then to the elevator and then the red, you will know. Is the exit for staff as they leave. This example also creates an area for staff to remove PPE and shower after the completion of their shift. Now, I’d like to turn it back over to Garth.
Garth Johnson
OK, thanks, Kevin. Obviously, we could do a whole seminar on some of these smaller concepts, but before we open things up to get feedback and to address questions, let me summarize some of the key points we talked about. We first acknowledge that addressing older, skilled nursing facilities requires confronting barriers. There are barriers within the industry overall and perhaps since these have been made more obvious with covered, this will become a time of change. That’s all our hoped. The challenge for us is for us to embrace this time rather than to shrink away from it. The place to start is not with your building, but with your care model. What is it that you’re trying to do? For example, we found that facilities managers are good allies in building projects, but it’s also very common for us to work with facilities staff whose vision of improvements largely consists of replacing old systems with a newer model that practically does the same thing. A wider vision is needed, and that’s why, as an organization looks to change, it will involve looking at programs, staff utilization and improvements organizational wide on top of the challenges posed by the building itself.
In fact, that’s where the whole process starts. We use the term areas of focus to describe services and priorities you’re looking to put in place and then densified. Seven We’ve heard from clients and industry overall and the reason why we highlighted that is that in our experience we found that different providers honestly have different priorities in terms of what they’re trying to accomplish. And so, as a result of that, there’s no single template that fits everything. And so, things like screening visitors, resident connection and visitation staff safety are going to be priorities based on the individual provider, and that results in a different building program and priority haven’t shared the idea to address infection control regardless of the size of the project.
We’ve found it helpful to look at H3C indoor air quality in three buckets and obviously this could be a seminar as a whole. The first is to open and optimize what you have. That’s the first step. The second is the point of function HPC systems in a focused reconfiguration, for instance, creating isolation rooms or visitation rooms. And then when an opportunity comes up, take advantage of it. When you have a project, make sure you do the mechanical systems well finished materials selection matters and Laura shared five key priorities to consider on projects are major, major encouragement is to be strategic.

Irving Stackpole Thank you, Garth, Kevin and Laura. You have covered masterfully the set of challenges that the audience, many operators, owners, managers are facing with regard to their physical facilities. These are the covid-19 we’d like now to consider questions from the audience.
Questions
Question: Many of the operators that. I my firm works with are challenged with regards to staffing challenges, with regards to the age of their properties, their equipment, and also challenged economically either a set of two or three interventions which your team sees as you look across the types of projects that you undertake, there are a few suggestions that you have that are both immediately effective and economical for this for this audience.
Kevin Kozak I mentioned that we’ve got some technologies that we’ve been researching, essentially trying to really vet. There are so many people out there that say, we can kill covid. And some of them, I think are some of them actually do that and some of them don’t necessarily have the science to back it up. But that’s definitely one because, you know, you mentioned staff and an isolation room that staff can go into because obviously you have residents that need to be cared for and that’s going to continue indefinitely. I think that’s one. And that’s a that’s one that anybody can do, whether they were doing a renovation or they were just wanted to increase staff safety and also other residents’ safety, because as we noted, if they’re in that facility, you want to make sure that you can keep the other residents safe, which is obviously what happened at the beginning of the pandemic. So that’s one I can think of. Garth and Laura, I don’t know if you have any other thoughts.
Garth Johnson I think that if I can add to that, I think before covid almost all of our work generally involved outside of the resident rooms, the focus was to address the front door, to address the community spaces, to address the dining area. So, there was a business has had an impact boom when you walked in. And that was really pretty much most of the time all the people were really looking for to address, obviously, with covered the realities of what is the how where does a resident potentially pick it up at it, particularly if they happen to be quarantined in their room, that it is expanded the scope of the focus of the traditional skilled nursing to the entire building. And so I guess my quick two cents would be to first to try and identify, particularly with providers being way down in their census. What are the critical things that we can be able to partner with them that can establish a clear message to the people that are looking to attract, as well as your staff and residents to enable them to be able to communicate?
This is what we’re doing as a result of what we’ve experienced and to be able to have a message that would be able to go out, whether that’s an isolation room, quarantine or other things like that, and then to establish a program that would enable them to start with a few things and then move on from there. I think we’re at a point right now that the whole overall health of the facility is going to continue to be just a high-level issue for a long, long time. And so the paradigm of kind of let’s dress up the interior look of the building is going to continue to be the reality. The buildings need to be made attractive for people coming in. But we have to realize that we’re fundamentally about health care. And that’s going to be key to be able to communicate a consistent message about what we’re doing to keep people safe.
Laura Sheehan Just to piggyback on what Garth said, you know, like you said before, we were focusing on areas those first impression areas to produce a wow factor. But the reality is that these residents are spending time on their unit for the most part. And a lot of them, while we want to get them out into the common spaces, they’ll be in their rooms a lot of the time and they take pride in ownership and in their room. That’s what they have now. That’s where they live. That’s their home. So it’s important to take into consideration all areas of the building, not just the wow factor areas, but where the residents are going to be resting and sleeping and relaxing, reading a book because that is their home.
Garth Johnson If I can add one of one of the things Irving as well, and that is I think the technology is rapidly changing in terms of how to deal with infection control that’s airborne.
You know, probably everybody in the audience is certainly aware of a point of use systems that were popular, that were used quite a bit at the beginning of the pandemic. And those got moved into systems where and probably all of us have heard of bipolar ionization and things like that. But literally, just as last week, Kevin and I came across a group that we’re now engaging with and just doing due diligence on, there is another way of sanitizing here that has a pricing point, which is lower than a lot of the systems we’re at. And if anybody’s interested in that, we’re really just starting to get it out. But there’s a new wave of stuff that’s coming in this group. They’re coming from the lab space. And that I think we need to continue to keep attentive about and that are going to enable us to help incorporate these kinds of solutions as far as the process continues. Technology is our friend here.
Irving Stackpole Certainly the image that we used at the beginning of the program about nursing centers being designed dinosaurs doesn’t mean that they have to remain design dinosaurs. And in these regards, technology, which in many regards nursing centers, got left behind in advance of technology. So maybe now it’s an opportunity to take advantage of the state-of-the-art applications that treat things like the air we breathe, the services, and then, as Laura was suggesting, colors and the like. See, I also want to observe that impact areas, as Flora was talking about and you were talking about the curb appeal area.
It has less. Importance now that we try to address the fear that exists in the general public toward congregate spaces, congregate places, and by making changes and communicating about those changes with our audiences, we can demonstrate that we understand that what their concerns are and that we’re addressing them in as constructive a way as possible.
Question: The new model, what a dining area would look like in the new model is what a dining area would look like.
Laura Sheehan So right now, obviously, because of covid, we’re seeing space restrictions and requirements. Tables have to be spaced apart. A lot of people are using barriers and guards. The there are many Plexiglas guards that have come out all different shapes and sizes that people are using to separate tables. And with increased testing and the vaccine coming out, I am hopeful that this is going to get back to normal eventually. But in terms of finishes and the look, I think that we’re going to keep moving forward with creating this really beautiful, almost hospitality. Look, you know, it depends on the facility in the client and also the location. Some people want a more hospitality look. Others want a more home like look. So, it really just depends on the vision of the client. But that’s what we’re here for. We listen to the clients dreams and goals and come up with the solution to make those happen.
Question: Thank you. You have a blank canvas or what is the ideal new SNF that you would build now?
Garth Johnson Well, I think it depends a lot on what it is that you’re trying to accomplish. My view is that certainly during this point, the either whether it’s a larger building that’s broken down into smaller, small houses or I would move in the direction of smaller congregate kind of living situations. But that is a big issue that really takes basically an organization to turn itself upside down in terms of the way in which it operates and to approach things of that nature. I think that coming and I referenced it broadly in terms of community-based care, is is probably the coming wave of where skilled nursing is moving as a whole. It is a radical change in terms of the way an organization operates. And but I think that’s what’s coming. That could be. And in the context of a larger building, Kevin mentioned the group that we’re with. And so, it doesn’t have to be a small house kind of thing, but it can be a congregate, you know, a larger congregate building that’s broken down into those sorts of things. And generally, you’re talking about a lifestyle. The other thing that Kevin didn’t mention, but the one of the major catastrophes that occurred was the absolute degree of isolation that occurred, know, and and skilled nursing facilities and literally the tragedy of people passing without having human contact, particularly from family members. And so being in context, where you’re in smaller groups, there’s a lot of advantages along those lines and getting actually getting back. Irving, to what you mentioned earlier in terms of the messaging part of the reality, for instance, again, here in Massachusetts where we’re based, is the current sniff infection rate is far lower now than the overall population. And yet that message is not getting out. And so organizations that are aggressively looking at the messaging that they have and then and trying to get a couple of their care model to it in terms of emphasizing those things, I think are the organizations that are going to do well. And then when they are able to make incremental changes or if they have the opportunity to do something broader and start from scratch, that would be a great opportunity to be able to change the whole narrative.
Irving Stackpole So it’s a terrific answer. I have to reflect on the fact that it really was a whoever asked the question, I’m sorry to say this is not your question, that the white can this white boy blue ocean question really has to start with one answer. Who are you trying to serve and what are you trying to do? And if you’re serving a jerry psych population that is far along in the trajectory of their illness in the course of their chronic illness, that population requires a very different space from a more ambulatory short term rehabilitation population. So, we really need to start with the population we intend to tend to serve.
Garth Johnson Now, if I can throw something else out as well, Irving, our organization there, at least right now. Well, we hope it changes. There are far more facilities that are looking to try and figure out what do I do with my existing buildings than are there are opportunities for people to be able to make changes. What we’re trying to do as a firm that has both design with Kevin Laura and their staff and other people is that we’ve been primarily oriented toward existing buildings. And part of the reason for that is, is that I think the architect community and I’m not throwing stones, but generally it’s a lot easier to think if I had a whiteboard, what would I do then? Think about if I have an existing building, what do I do? And so, we’ve been oriented more toward that, although we are privileged to have the opportunity to be able to work in new spaces just because I think that’s where the industry as a whole is going to go in terms of addressing that. I think the other thing is, is that, you know what I would say and we’ve talked enough between the two of us to know that we’re kindred spirits here, you know, that that the system as a whole needs to be rebuilt.
And if we have the opportunity to be able to do that and unfortunately, here we have a state organization that that I’ve been involved in that is actively trying to figure out what do we do instead of waiting for the feds or the state to say, here’s what we think you should do with your building. You instead basically start saying, let’s aggressively try and figure out what are the key things we can do and then honestly go to the state and say, here’s the three or four things we should do with most of our buildings to fund that would take blank and to be and let’s approach that rather than waiting for the regulatory officials to try and jam it down our throats and usually have that guidance be misguided because they don’t understand care. And so, my encouragement to all of us listening would be to get engaged with groups that are looking in that direction related to what we can do with our with our facilities related to HPC, related to the things that are directly infection control related, and then and get in robust discussions about the sorts of things needed. And then let’s put it on the table and seek to see if we can get funding and get an audience that can address some of these things so we can get where we need to be. I think we need to be as a as an industry leaning into that. Yes. And not just waiting, hoping that somebody will give us a rescue.
Irving Stackpole That was really thank you for that. And that was really the motivation. That is the motivation behind this webinar series is to start these dialogs, is to start the discussions. And across the country and even internationally, we know there are things that need to occur. We can no longer kick the can down the road. There’s a big pile of cans somewhere. We have to address these issues now. And to you to your point, back on one of the first slides, we know that we need a lot of different stuff, but we have to start somewhere. So, we hope that this is a good start. I think we have time for another question.
Question: Kevin, are the strategies that you were talking about gesturing infection crises all the time, especially in visiting rooms?
Kevin Kozak I think specifics to the visitation rooms that really is focused on specific to covid and pandemic just because of the idea of keeping residents outside or keeping visitors outside the neighborhood, normally you a visitor would come in and they go visit their loved one within the unit. Keeping them off the neighborhood, I think is a good idea. And I think that really sprung up as a result of the pandemic. And also, Garth and others mentioned some of the regulations know there was a period of time where even if you wanted to do it, the state or wouldn’t even let you visit anyone, even if you had done these things. So, I think for the most part, I think it’s certainly something that as we move along, I think it’s a good idea in general. But I think that concept really started because of what we were saying. So, I don’t think we would have ever even thought of creating a visitation room a year ago. So.
Garth Johnson Yeah, and I think, Kevin, just add on to your comment. Most of the people that we’re talking to, unfortunately anticipate that we’re going to have we’re going to have other issues like this that are going to continue. This is not going to be an issue where we’re done and everything’s back to normal.
Irving Stackpole Normal, which is really good anyhow. Nobody was waking up in the morning saying you’re going to a nursing home today.
Question: I believe covid has been difficult in SNFs due to more airborne transmission than we know today in the zone approach for larger facilities. How do you see managing staff, visitors and others who need to enter multiple zones on the same day? Are you confident that the zone approach can isolate potential, the individuals in question?
Kevin Kozak, I don’t know about, you know, globally, the idea of the different zones. One is, is that we would then not have cross contamination. So, if you had a public zone, you’re not going to take the air from that public zone and you’re going to put it into the semi public or private areas. And you’re going to think about buildings in a different way than we’ve done it. And Garth alluded to it before. The old model is you dump fresh air into the corridor and it just kind of goes where it goes. And we can’t think like that. We need to really think about where that air goes. So, I certainly can’t say one hundred percent. Oh, yeah. There’s no way that air is going to get from because if a person goes from the public area and they go all the way in, then that person is going. That being said, you by limiting into the zone approach, you’re limiting the exposure because you’re that that air isn’t going to get into the next zone and into the following zone. And by having created that and it’s just it’s just a different approach than we’ve really ever thought of. And I think it I believe it will have a big effect on systems of health.
Garth Johnson You know, I think the only comment that I would make along those lines is the reason why I responded the way I did in terms of operational is some of the person centered care concepts are things like consistent assignment, where staff are consistently coming back to the same group of small groups of residents. Self-directed teams is a is a similar person centered thing. And so, the operating model, if an organization isn’t pulling them, well, then obviously zoning isn’t going to work. And so, again, I think, Kevin, this goes back to your hierarchy of care and thinking about the reality of this. The building relates to the care model and your organization model, and those things have to be symbiotic. And in terms of how it works.
And so, when we have the opportunity to work with the client who really knows how he wants to do it, and the systems can be designed to just support that. And the difficulty that were occurring right now in in many of our facilities, our buildings are built toward staffing approaches, which nobody is doing to these days. And so everybody’s fighting against their building. And so, we can just view it as a war that you have to kind of climb Everest either quickly or slowly back to kind of get the building to support the approach. That that’s the mindset, I think.
Irving Stackpole Right. In addition to fighting against covid, where we find ourselves fighting against time, our time has just about run out. My hope is my sincere hope is that wherever you are in the audience, geographically, program wise, facility wise, that this is really just the beginning of the discussion. This is the way to launch serious conversations about what needs to occur in the sector in order to save it so that those who need it will be able to access it. I want to personally thank Garth, Kevin and Laura for participating in this and for all of you for attending so carefully.
Resources
- Williams, B. Failure to Thrive? Long-Term Care’s Tenuous Long-Term Future.
See: https://scholarship.shu.edu/shlj/vol43/iss2/3/ - Stackpole, I. Bridging the Divide: Transitions to Cross-Continuum Collaborations in Healthcare.
See: https://stackpoleassociates.com/transitions-cross-continuum-collaborations-healthcare - Who Cares? The pandemic shows the urgency of reforming care for the elderly. The Economist.
See: https://www.economist.com/international/2020/07/25/the-pandemic-shows-the-urgency-of-reforming-care-for-the-elderly - Coronavirus Commission for Safety & Quality in Nursing Homes
See: Final Report of NH Commission Public Release Case.pdf - Davidson, J. The American Nursing Home is a Design Failure. See: https://nymag.com/intelligencer/2020/06/the-american-nursing-home-is-a-design-failure.html
Stackpole & Associates is a marketing, research & strategy consulting firm focused on healthcare and seniors’ services markets. Irving can be reached directly at istackpole@stackpoleassociates.com.