


Date: 6th August 2020
To watch the recording click here
Register to download the webinar presentation.
Transcript
Marketing Fawlty Towers: 4 Ways to Restore Long Term Care
Irving Stackpole
The topic today is long term care, which is at a crossroads both in the United States, the U.K. and elsewhere. I’m using the image of Fawlty Towers, the famous or infamous John Cleese program comedy program built around the care home in the United States and its adventures, or should I say misadventures.
 What I hope to talk about today is the current situation in care homes and long-term care, focusing particularly on the UK. Talk about some myths. one myth in particular about aging. Talk about, of course covid-19, which is at the center of the current crisis in the sector, review likely recovery models and some scenarios and more importantly are very importantly effective responses. How can managers in the sector respond effectively in this during this crisis and immediately afterwards and focus on those possible actions on the four strategies that we’ve seen work in other markets and in other circumstances when there’s challenges.
What I hope to talk about today is the current situation in care homes and long-term care, focusing particularly on the UK. Talk about some myths. one myth in particular about aging. Talk about, of course covid-19, which is at the center of the current crisis in the sector, review likely recovery models and some scenarios and more importantly are very importantly effective responses. How can managers in the sector respond effectively in this during this crisis and immediately afterwards and focus on those possible actions on the four strategies that we’ve seen work in other markets and in other circumstances when there’s challenges.
The first myth I’d like to address has to do with aging itself. There’s quite a bit of humor in this photo, but there’s quite a bit of buzz associated with the size of the aging population and the number of individuals in it.

This myth has been promoted widely. The myth is that there’s just a lot of age targeted, age-appropriate consumers in the sector. Well, the truth is that in England and Wales and the situation in the United States is very similar. The primary age at which consumers begin to more aggressively consume long term care services is eighty-five years of age.
If you look at the number of live births in the United Kingdom in 1935, you can see that that’s when someone in 2020 would be 85 years of age. You can see here that in 1935 live births in the United Kingdom, we’re at a low point and they remain at that low point for quite some number of years, 7 or 8 years, and then they begin to increase again.
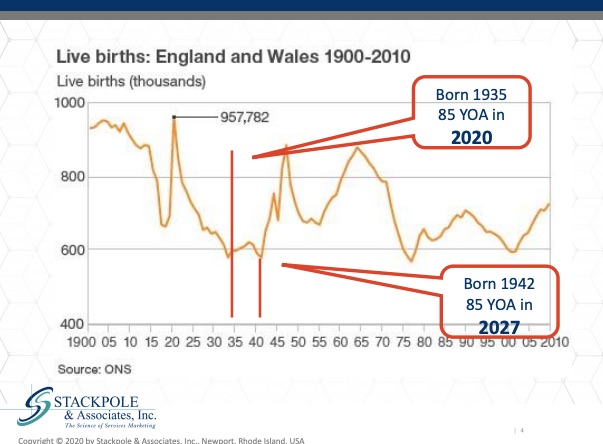
It isn’t until 1942 that the live births in the United Kingdom started to pick up again. Between 2020 and 2027, we will be experiencing more of a drought, more of a dearth in age qualified consumers in the long-term care markets. Now this is often overlooked or not discussed at all, even in academic papers. This is a dramatic oversight. The important thing for us is that the market for long term care services in the United Kingdom and in the United States, even before covid hit the market, was terrible. It was bad before the pandemic and now the pandemic has ravaged congregate care in the United Kingdom.
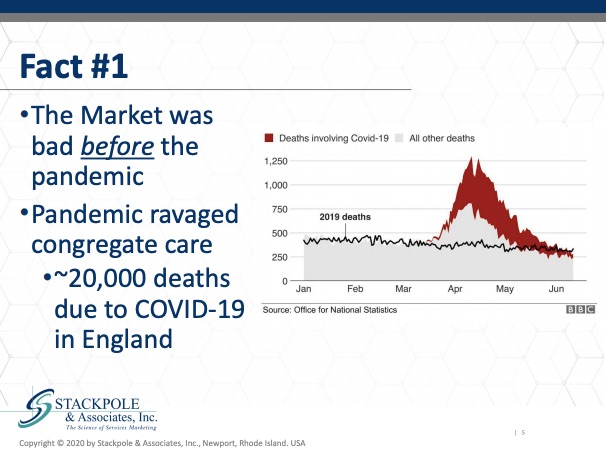
And you see from an ONS graph that appeared in the BBC, these, quote unquote, excess deaths in the dark red hair associated with covid in care homes in England and Wales, and actually one would need to do a very careful analysis of above the benchmark line of 2019 deaths to determine which component of those are actually traceable to covid-19.
Perhaps covid-19 wasn’t mentioned specifically on the death certificate, but actually there was a primary contributor or actually the main cause of death. It’s a significant crisis. The issue with the crisis, of course, is that it’s an unexpected event. But what damage does the crisis do to our brand? What is the brand of long-term care in the UK and the United States, in the United Kingdom, Wales, Ireland and in the United States? Well, the brand is indeed Fawlty Towers. It is a negative metaphor in general. Fact number two, the brand now is damaged. We’ve heard so many times from so many clients and its so many conferences, forums, newsletters, research reports, phone calls: It’ll never happen here. We have a great reputation. Families love us, local authority love us. We know what to do. My team can handle it well. Truth is that this is a kind of seismic change in the negativity with which the public views congregate long term care and the news media.
As you can see from the foreign news article here, the feature piece that appeared in early May, this is just a field day for the media to sell negative stories about the sector. So What’s different in this situation is that the entire sector is under siege. This is prompting or stimulating latent guilt in our cultures about not caring for grandmother at home. It has no end in sight.

There is no specific end that one can point to and the fulfillment or production is threatened. By that, I mean the staff are equally threatened in care homes and nursing centers. That in turn has the corollary or the obvious question who wants to work for you? Who would want to work in a sector that’s being so ravaged by the muck, by this disease so that recruitment and retention is it is an enormous challenge in. Regular circumstances and now in this crisis, it’s accentuating or exaggerating the negative impacts of the economic model, it’s bringing home the fact that in care homes and nursing centers in the UK and the US and other places is a very mixed inventory. It’s difficult to be consistent and have consistent standards when the inventory ranges from very small care homes with only a few units to very large centers that are custom built. The other issue with recruitment and retention is the regulatory burden.
It’s very difficult environment to work because of the regulatory component. We just learning recently that the public accounts committee in the U.K. is publishing its review of the need for guidance in the long-term care sector, much overdue. But this is the type of regulatory scrutiny that will result from this covid crisis, which has been needed for some time, but which has the risk of holding significant, untoward, unexpected and unpleasant surprises. It also has the potential for creating some very positive changes in the sector and the role that we as providers and as organizations, the role we can take in directing that I think is tremendously important. The other thing in recruitment and retention is this issue around negative cultural bias toward care homes, toward long term care, toward nursing centers. This has a direct impact on recruitment and retention as well, making the job of finding and keeping qualified staff, qualified personal care attendants very, very difficult.
In the UK, it’s a pretty big sector and there’s about one point two million individuals who work in long term care. This includes nursing homes, domiciliary care, community care and care homes in general. You can see that the vast majority are, well, a majority, 610 thousand work in people’s homes. It’s a large group. It’s a diverse group, and it’s a very low paid wage group.

You can see here from data looking at job losses in the United States, in the United Kingdom, which job, which payroll cohorts, which pay rate Streator are being most impacted by covid. You can see that the low pay wage groups are being disproportionately impacted by unemployment at this time. We can see that the means of production, which is another way to say that to our staff, they are our means of production and long-term care. They are being outsized, impacted in a negative way by the covid-19 crisis.
The Skills for Care did a survey pre covid-19 and looked at the difference between leavers and stayers in care homes and in long term care, the adult social care workforce.
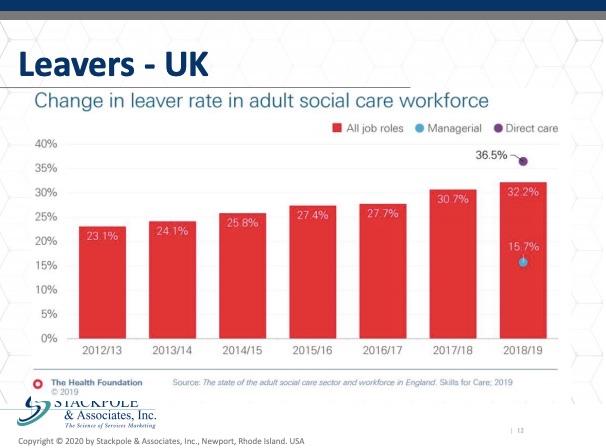
We can see that there’s a disproportionate and growing number of individuals leaving versus staying. So, it’s extraordinarily important to zero in on this component. As we look at issues such as regulatory burden, as we look at issues such as the economic model, to look at how adult social care, long term care, congregate care can become more competitive in the workforce, in the labor, in the labor markets.
Summarizing about staff, we have a situation where we’re struggling for recruitment. It’s difficult to retain staff under the current. It was difficult before covid and it’s even more difficult now as unemployment surges in other situations during economic downturns or regular standard run of the run of the mill recession. You’d look at unemployment growing and say, well, is this an opportunity for me to recruit from an unemployed group of individuals in my local marketplace area? But the question becomes it is long term care an attractive alternative for suitably qualified, motivated individuals who become unemployed?
That raises the question of how we communicate the relative advantages, disadvantages and features and benefits of recruiting staff to work in long term care. There’s been some interesting work research done on this, but we don’t see these research reviews, these peer reviewed studies. We don’t see them being implemented by care providers the way we hope they should be and could be. Struggling occupancy, struggling recruitment and retention. The economic model is struggling. We have old inventory, onerous regulatory burden and negative cultural battle. Pretty chipper assessment. I’d say overall it’s quite a quite a situation. So how do we recover? Well, in among the models of recovery. We look in general at economic modeling to see what’s likely and in this. Current situation where the responses, the public health responses to the disease have been remarkably inconsistent between and among countries, what we see in the United States, between and among states, what we see most likely is a recovery model where we begin to recover and then there’s stabilization or deterioration and then we begin to recover still further and there’s further stabilization or deterioration, etc. And that’s the way we see this recovery occurring.
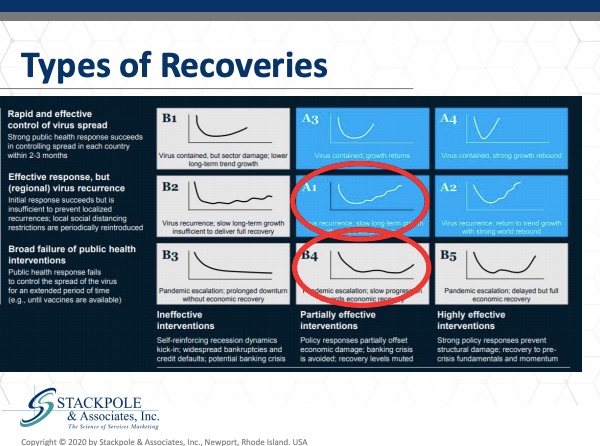
Alternatively, we could see recovery and then another wave, people haven’t been really talking about the second wave of sars-cov-2 the novel coronavirus, but that is looming. Most of the discussion has been about what’s occurring still in the first wave. But we have a second wave of the virus to anticipate. We can hope we can pray that there will be a vaccine available and effective treatments available. But the fact is that this pandemic will follow the path of previous pandemics and there will be a second wave, which may mean that the type of recovery we have will look like before rather than a one. The factors that will be important to rebuilding and restoring the brand of long-term care post covid have to do with the acceptance of congregate, long term care and long-term care overall have to do with acceptance of it in the cultures.
In the U.K. in particular, how well is long term care in particular? Nursing care, adult social care, how well are they accepted and the flip side of that is to what degree it’s actually utilized and that’s the term penetration. we look at that carefully to see what impact acceptance will have on penetration. There are always trade offs as tradeoffs between the risks associated with moving into or considering utilizing long term care. There’s always a tradeoff between doing nothing, what the status quo is and the advantages of accessing or utilizing long term care.
From a sales and marketing point of view, from an acceptance penetration point of view, long term care is a solution that’s almost always pitted against the status quo. No, no. We can take care of this. The tradeoffs are between the accessing long term care and the status quo. There’s also, as we already alluded to, the issue of government and regulatory intervention. It’s an enormous challenge. Governments across Europe and in the United States do not have a very good regulatory monitoring and surveillance schemes for long term care. The reasons for that are multiple but have to do primarily with the relative importance of long-term care in the monopoly of issues that governments need to deal with, and frankly, long term care has been relegated to secondary or even tertiary importance. But yet the regulatory intervention, an intervention loom. That said, whenever something bad happens, it makes it into the press or makes it into a politician’s front of mind awareness.
That’s what we need to be wary of and need to be concerned with. This is among the things that we as managers, we as operators and or academics have an opportunity to influence going forward. We will probably see more onerous regulation. One can hope, one can plan, one can push back. But I believe we’re going to see more onerous and perhaps even more inconsistently applied regulation. One of the issues in the UK and in the US has been that the regulatory body in the UK that you see that they have applied the regulatory standards with a high degree of a variance. How homes in Lincolnshire are evaluated by the authorities is very different from how they’re evaluated in another location. The difference between how the regulatory regulator looks and assesses care, home outcomes, care home standards in one place is highly variable and that’s certainly a problem and increases the burden for us who are attempting to operate and work within those regulatory standards.
The one issue that hasn’t been talked about very much, I think some private groups are beginning to talk about this and address the issue of liability protection and exposure in the insurance markets. Covid-19 is opening up this issue about liability, liability protection, malpractice protection from lawsuits. We’re just beginning to see the ripples of these impacts in management and in ownership of the properties, the assets in the sector.
Post covid-19, the likely recovery models are going to we’re not sure about the depth length and the shape of the recoveries. I see two possible scenarios. Scenario one is that the sector is rebuilt and recharged. There’s certainly a number of people who are looking at what’s needed in the sector. Innovative ideas are circulating, and I think there are lots of ideas on the table. But what I’m concerned about and what we should all be prepared for is that it could be ravaged and further relegated when so many issues need to be tackled. So many political hot potatoes, hot subjects are to be dealt with.
Will long term care homes and continuing care, will it be further relegated to the dustbin of public service issues? I’m not sure, but I don’t want to leave without talking about what it is that we can do.
These are all concrete steps which we’ve seen work. We’ve seen work in multiple places and which we’ve imported from other sectors when necessary. So not what we can do. No one in our operations, regardless of where they are, is we can take responsibility for the messages, we can take responsibility for the narrative. I believe strongly that we need to move and shift the story line around long term care and the value of long-term care to the community, the value of long-term care to its consumers and its residents and the consumers and include the families. We need to take charge of that. I don’t mean portraying we as victims because I don’t believe in the long run. Victimhood will shift the narrative. It will not create any long lasting or durable change.
While it may garner immediate sympathy or empathy. It will not, in the long run, reposition the brand of long-term care as being important, as being valuable, as being a good, socially sensitive and an exciting and stimulating place to work. It won’t change any of that.
We need to take charge of the narrative and we need to tell the stories and show the images. I know this is particularly brought in the UK with its tenuous relationship with the news media and news loved ones. News media and news outlets are always looking for the negative side of a story because it is, unfortunately, the negative stories that sell newspapers. The more clicks, the higher the value of the ads that get placed in those channels.
The negative stories do indeed garner the greater attention. But we have a responsibility to develop a very consistent, regular drumbeat of positive stories and important contributions that long term care is making to the communities we serve. What we can do? We can fortify, protect and defend the market share that we have now, and one of the things that we absolutely need to do in the long-term care sector is we need to review our digital assets.
We have as providers, owners, managers, as consultants to the sector. We have been neglectful of websites, of newsletters, of our Facebook presence, and this is showing up to our detriment now in a crisis when families are relying on these digital channels now more than ever in the crisis communications mode, which is where we are, we have a responsibility for communicating and managing the story with families, employees, our fellow providers, local authorities and other stakeholders. We it’s up to us to manage the message. We must accept and understand fear, fear is operating at a more significant level now and will continue to be a blatant or overt factor in consumers and their advisers and customers and consumers point of view about long term care going forward. So even in situations where there have been significant infections, where there’s been significant death, where there’s been significant negative stories, we need to take charge of those stories and begin to address directly address what we can do about fear. There’s very good research about communicating in environments that are fearful and how we can manage the messages to assuage or reduce the levels of fear in the audience.
Finally, we need to do a much better job at service ever recovery. And there’s a science around service error recovery. And you might say categorically that there has been a service error in long term care, and it has been our inability to properly manage the covid-19 outbreak. Many care homes, many nursing centers, many nursing homes, many domiciliary care agencies, many congregate care centers have done a wonderful job, have led the way. And we need to do a better job of understanding and communicating about those situations and learning lessons from those providers. But we also need to adopt a more scientific approach to service their recovery. And here are the keys to service their recovery.
First of all, you’ve got to know when an error occurs, and service errors can occur in a variety of different ways. But you need to be if you’re the manager, owner, operator, leader within your organization, those errors need to find their way to you. In many cultures, many organizations, front line workers hide the errors out of fear of retribution, of not wanting to look good or afraid of what the outcome will be. Well, that doesn’t help anybody. You need to be able to identify the errors. Then we need to apologize. Very large research in the United States has shown that the major reason nursing centers in the United States get sued now legal action taken is because nobody apologized. When you ask the nursing center managers why they didn’t apologize, it was because they were afraid of getting sued. This is a very negative cycle that needs to get broken with a simple apology and an offer of a solution. We need to apologize and offer a solution, then do the solution, do what you say you were going to do and then later on remind those involved of what you did and how you address the situation.
We have terrific resources on our website. We have a presentation called Satisfaction is Cheap, Loyalty is priceless. The drills down into the science, the behavioral science associated with effective service that are covering this is very well researched and grounded in business, in the business press and in academic research. Item number three is we need to get serious in the sector about efficiency, efficiency is a very specific word and it’s not a code name for its efficiency is not a code for eliminating staff, which is very often what efficiency is taken to mean, all in efforts to improve our efficiency. We’re laying off staff. No, that has nothing to do with efficiency. That’s cutting costs and that’s removing overhead efficiency, its outputs for inputs. It’s not its efficiency is related to productivity, but productivity is not equal to staff reductions. You don’t become more productive by reducing your staff. You become more productive, productive by having the right person do the right job at the right time with the right materials and to do the job right. We did a major survey among care workers, front line care workers, about what the difficulties and challenges they had in providing morning care. You know, personal care attendants go around and do morning care with individuals, the basics of grooming, toileting, cleaning, bathing, that type of thing. What we found in hundreds of interviews, what we found was that the personal care attendants who had difficulties, the 80 percent of the time, it was because they didn’t have the washcloths, the basins, the soap.
When we looked further, it was because other more experienced and more cynical care attendants had sequestered that stuff, had staff that stuff away so that they had a secret pile of this stuff put away. And why did they do that? Because they had had the experience that the staff who reported difficulties had had. And this whole thing was just a mess. And it got fixed. It got fixed by talking to the front-line staff. Efficiency has to do with the right person, with the right qualifications, doing the right job at the right time, with the right materials and doing the job right the first time. Efficiency is often talked about in the context of technology and information. Long term care is the land, the technology and information systems left behind, unfortunately.
The technology that’s available today on tracking materials, tracking actions and individuals’ pathways within a within a care setting is very good and it can improve technology. But we mustn’t wait for the money or the advancing technology in order to look at efficiency, to talk to the front-line care staff, to talk about how we can improve efficiency and make the outputs more effective for the inputs. The fourth thing that we can do is differentiate. In the current market, we need to defend, fortify and emphasize value the importance of the benefits being derived for the care being provided.
We need to protect, defend and four to five current staff. We need to do better with service are recovery. These will help innovate for efficiency and to differentiate our service in the local marketplace area vis a vis other potential provider as well.

In conclusion, the current situation is that we’ve got some myths about aging. We’re in for another six or seven or eight years of declining age, qualified the size of the age qualified consumer market. The likely recovery models and scenarios will be challenging. Our best and most effective response to this is to take charge of the messages, take charge of what we can do within our organizations to improve efficiency and effectiveness. That is the message that I hope to leave with you today.
QUESTIONS:
QUESTION: What do you mean by taking charge of the narrative? How can we do that?
That means you don’t wait for the media to show up at your front door to begin to submit stories and invite people from the media, from the community to talk publicly about what’s occurring in your community, the positive stories in every long-term care setting that I’ve visited, and I’ve been in thousands of them. There are serious people, sometimes funny people, but earnest professional people doing what they believe is the right thing for them for them for their charges, for the people for whose care they’re responsible. We need to get those stories out. There have been some extraordinarily clever things done, for example, about keeping residents in touch with and in communication with their separated, physically separated family members. Those stories are wonderful stories, some of them exceedingly clever. That’s what I mean by taking charge of the narrative. You don’t need a public relations firm. You don’t need an advertising agency. You need to think about what some of the extraordinarily clever things or persevering things or heartwarming things are, funny things that are occurring here. How can we turn this into a message that’s sent out presented to our communities in order to show the value of what’s occurring through our service? I hope I’ve answered that question.
QUESTION: How can we improve out PR when I cannot afford a professional agency?
I believe that the steps that we should be taking now are to create lists of media contacts in the press, both electronic and print and the local, the local authorities, the media, everyone, our stakeholders.
We should have their email addresses. We should have their preferences, especially to the media, the print media, what their preferences are. And when we create these stories, when these stories come to us about something extraordinarily effective that an employee or staff member has done or some heartwarming connection that a resident has made, we should be making these stories with people’s approval. Of course, we should be making these stories and images available to those members of the press, to those digital news outlets, through our newsletters, through our digital channels. We should be making those messages so we can start now without investing in a PR agency, a professional firm. We can do those things today and we should be doing them well.
QUESTION: which is what if the negative press has already surfaced and people are biased due to input due to the information.
There are two components to that. There’s a negative story about your nursing center. That’s not you’re not referring to the general cultural negativity, but there’s a very specific negative story about your center or about your service. We have a PowerPoint presentation and I think a webinar on crisis communications on our website, and I would refer the person who asked that question to that resource. But the basic principle is, first of all, you get out up in front of that story, you as the leader, take charge of that story by being visible and responding to it. Even if you can’t say much because of GDP or because of Hip-Hop, because of the sensitive nature of identities of the individuals, you can step out in front and say this has occurred. We are working with the local authorities.
Our commitment remains to the health, well-being and success of our staff, our residents, our patients, our consumers, and we will do X, Y and Z. We will be back in touch. We will communicate as we are able. And any questions should be directed to me, to the leader. I’m ready and able to answer because our commitment is to our employees and staff. So. You take the negative and you make I call it a sandwich, you make a positive statement, you describe what occurred to the extent you were able, and then you repeat your commitment to the well-being of those you’re caring for. So that’s how you get out in front of a negative story that there’s far more to it than that, obviously. And I would refer you to our website where there is the webinar on crisis communications.
QUESTION: In my market, a person can make more money work in McDonald’s than a nursing home and they get all the Big Macs they want. How would you recommend finding your way to the nursing facility with such a competition?
Whether it’s whether it’s McDonald’s or a Tesco, the long-term care providers are competing for the same front-line workers as are those other service intensive or service-related sectors. By the what the research has shown is that there are specific psychographic profiles of individuals who would prefer to work in a nursing center, who would prefer to work in domiciliary care, who would prefer to work at a care home as opposed to a Tesco or a Kroger’s or a McDonald’s. Our job is to use the research to find those people. And we find those people by using the trigger words that will attract them preferentially to our recruitment efforts as opposed to McDonald’s recruitment efforts. Because what McDonald’s and others, what these high volume, high churn employers are doing is they’re working on the numbers. We can’t work on the numbers because we don’t have that big a budget. What we have to work on is we have to work on the psychographics, so we have to carefully segment.
The first step in doing that is to talk to your best employees. You talk to your best employees, and you understand why they like it, why they’re so loyal, what they liked about it when they first started, why they stayed and used those words, those key words in an Internet search way of speaking either in print or online promotions in order to preferentially attract those staff who would prefer to work with you as opposed to a McDonald’s.
QUESTION: Will families recover that trust of their homes after.
First of all, there is a baseline of demand in the long-term care markets that’s driven by physiology and by clinical conditions. There’s a baseline demand that really will not go away. And that is, we all know neuromuscular disorder, dementias of various types of disabilities of other types. There’s a baseline demand that will endure above that baseline demand. There’s quite a bit of variation in acceptance and penetration, as I talked about. Families will respond to. The question about long term care based significantly upon what’s referred to as personal access, so what stories have families heard through their networks or through the media they consume? What stories have they heard about long term care?
If in your marketplace area, the stories that are running are primarily negative, the messages and predispositions that the families will have will be fundamentally negative. If you can counterbalance those with positive stories, if you can share is that I was attempting to explain it earlier. I hope to some degree of success, if you can share positive messages, take charge of the narrative within your marketplace area, then there’s a chance that the families will have absorbed some of those messages. But the background of fear can be overcome by reporting very specific information and how you have responded to covid when the consumer asks you about it. There’s a very specific rigor associated with that. But in general, families will learn to fear less as the news cycle shifts away from the negativity in care homes and shifts toward, frankly, toward other topics already. There are signs that consumers are becoming weary of the negativity in messages around care homes, nursing homes, around health care hospitals in several marketplace areas. I believe as the news cycle shifts, this the negativity will abate. But we as the taking responsibility for the messages need to understand, it probably won’t go away completely. For years.
QUESTION: Most of the so-called service errors are just because of staff shortages. How can we recover from this?
So serious errors occur in part because somebody doesn’t answer a call or someone who’s taking care of Mrs. Jones gets a call that something is happening with Mrs. Smith that’s more urgent and has to leave Mrs. Jones to go attend to Mrs. Smith. And then when the carer, the caregiver returns to Mrs. Smith, maybe she was longer than she told, she wants to be an optimist, she said, Sorry, dear, I’ll be back in 10 minutes. And it’s fully 25 minutes or longer. When the caregiver comes back, her first instinct is to apologize, which is good. Sorry it took me so long. But then she wants to make an excuse. She wants to give a reason why she took so long. The simplest thing to say is we’re short staffed today and that’s an incredibly bad thing to say, even if it’s the truth. Staff must find other things to say, so in-service error, recovery, the first thing to do is to attempt to prevent the error in the first place.
If the error is upset around being short staffed, where did families or. Patients hear about being short staffed. They heard it from the staff, so the first thing to do is to make sure that that that is that does not occur. The second, looking at the steps associated with service, their recovery, the first step is to say, I apologize. The second step is to offer some solution. You know, when I leave here, when we’re done here, getting you dressed, Miss Smith, I. I feel badly that you waited as long as you did. I know you like that. That ginger tea. I’m going to go get you a nice cup of that ginger tea. Then the caregiver goes and gets a cup of ginger tea, brings it back and reminds the consumer here, dear, what I really did feel badly that you had to wait so long. Here’s that cup of tea that I promised you. So that’s how that gets handled. That’s how service recoveries that are associated with the fact of Short-Staffed become get addressed.
Resources
- Care Homes: Consumer Research. Ipsos MORI report for the CMA, August 2017
See: https://assets.publishing.service.gov.uk/media/599d9563e5274a28b5790976/ipsos-mori-care-homes-consumer-research.pdf
- Comas-Harerra, A. et al. The Long Term Care System for the Elderly in England. European Network of Economic Policy Research Institutes, May 2010
See: http://www.ancienlongtermcare.eu/sites/default/files/ENEPRI%20_ANCIEN_%20RRNo%2074England.pdf
- Sion KYJ, et al. Themes Related to Experienced Quality of Care in Nursing Homes From the Resident’s Perspective: A Systematic Literature Review and Thematic Synthesis. Gerontol Geriatr Med. June 2020
See: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7318818/
- UK Parliament, Public Accounts Committee. “Slow, inconsistent and negligent approach” to social care in the pandemic. July 2020
See: https://www.kff.org/report-section/covid-19-and-workers-at-risk-examining-the-long-term-care-workforce-tables/
Stackpole & Associates is a marketing, research & strategy consulting firm focused on healthcare and seniors’ services markets. Irving can be reached directly at istackpole@stackpoleassociates.com.